Some common tools when dealing with airway in trauma
Airway Management
Airway management in trauma is primordial if the paramedic is unable to have airway access the patient has a high chance of respiratory arrest. Causes of airway obstructions during trauma can include:
-
Loss of pharyngeal tone due to decreased LOC, TBI or shock (most common cause)
-
Posteroinferior displacement of a fractured maxilla parallel to the inclined plane of to the skull base that may block nasopharyngeal airway
-
Fractured or exfoliated teeth, bone fragments or other foreign bodies
-
Hemorrhage
-
Soft tissue swelling and/or edema as seen in anaphylaxis
-
Direct trauma to the larynx and trachea that may cause swelling in the adjacent structures such as the epiglottis or the arytenoid cartilage.
Given the multitude of possible airway obstructions that can occur from trauma, is it important to keep it patent? Keeping an eye on the following signs of respiratory distress will help the paramedic properly identify and treat the patient.
-
Laboured or rapid breathing
-
Intercostal muscle retractions
-
Stridor
-
Skin color change
-
Wheezing
-
Nose flaring (Especially in pediatrics)
-
Sweating
-
Obvious signs of airway obstruction such as impalement or intrathoracic perforation
Available tools
Depending on where you work, different tools for airway management are available, the NPA, the OPA, the crico and the ET tube are classics when it comes to airway management.
NPA
A nasopharyngeal airway is often used for patients that have intact gag reflex, trismus or oral trauma. It can also facilitate suction in a patient with a weak cough. It’s composed of a flexible tube with an angled ending and a larger top body.
Sizing
The sizing is done by measuring the tube from the tip of the earlobe to the corner of the nose. The internal diameter (ID) is given in mm and is usually 6-7 adult female and 7-8 for the adult male. A quick way to size it up is to use the patient’s pinky finger as a means of choosing the right ID.
Insertion
The tube must be carefully lubed and sterile. With the bevel facing the septum, insert the tube following the natural curvature of the nasopharyngeal airway. The tube is then rotated 90 degrees, where it should lie in the posterior nasopharynx. The nasal of choice left to the discretion of the paramedic according to which one is more patent depending on which nare is more predominant in the patient. Be aware that if the patient has a septal hematoma, septal deviation or any other congestion such as blood or nasal vasoconstriction. In this case, use the most patent nare.
Contraindications
-
Basilar skull fractures
-
Nasal fractures
-
Coagulopathy
OPA
The oropharyngeal airway is the noninvasive airway management tool of preference. Is secures the airway more adequately than the NPA. It is composed of a color-coded plastic tubular channel that lifts the of the posterior pharyngeal wall to prevent airway obstruction. It also assists in oropharyngeal suctioning if needed.
Sizing
The sizing is done by measuring the plastic tubular channel from the corner of the mouth to the edge of the mandible.
Insertion
In adults, the insertion is done with the OPA concave pointing towards the palate. As the paramedic inserts it, a clockwise 180-degree turn is done until the OPA resides completely on top of the tongue. In children the insertion is done without the 180-degree turn, it is inserted convex with the tip of the OPA pointed downwards.
Contraindications
-
Intact gag reflex
-
Oral Trauma
-
Airway obstruction
Cricothyroidotomy
A cricothyrotomy is used only when all other methods such as ET tube fail or are contraindicated. It is the last resort. It an emergency trauma setting, the most common method is needle cricothyroidotomy, which involves the insertion of a 14 gauge or greater angiographic catheter into the trachea through the skin and the cricothyroid membrane.
Sizing
In trauma setting the sizing is not done. A single angiographic catheter is a “one-size-fits-all. However, in a surgical setting, sizing is important.
Insertion
The patient should be placed supine with cervical immobilization if needed. Apply lidocaine (if indicated) and prepare a sterile field. Identify the anatomical location of the thyroid membrane and the cricoid cartilage as well as the cricothyroid membrane in between. Attach a 10-ml syringe with a 5-ml saline solution to the angiographic catheter and direct it caudally at a 45-degree angle. As the needle is advancing, apply negative pressure to the syringe, a distinct pop can be felt as the needle advances through the cricothyroid membrane. In addition, bubbles should appear as you are carefully withdrawing the plunger to check for air. As the catheter is advancing, withdraw the needle. Once done, attach the jet ventilation device, and ventilate at 40-50 lb per square inch or 15l/min. If that device is unavailable, you may attach a 3-ml syringe to the catheter and place an endotracheal tube attachment, this will allow the paramedic to ventilate with a BVM.
Contraindications
-
Should only be kept in place for 40 minutes after which CO2 accumulation can become deadly especially in head trauma patients. A permanent tracheostomy should be placed soon after the needle crico.
-
Other methods available such as King LT, Combitube, ET tube, and etc…
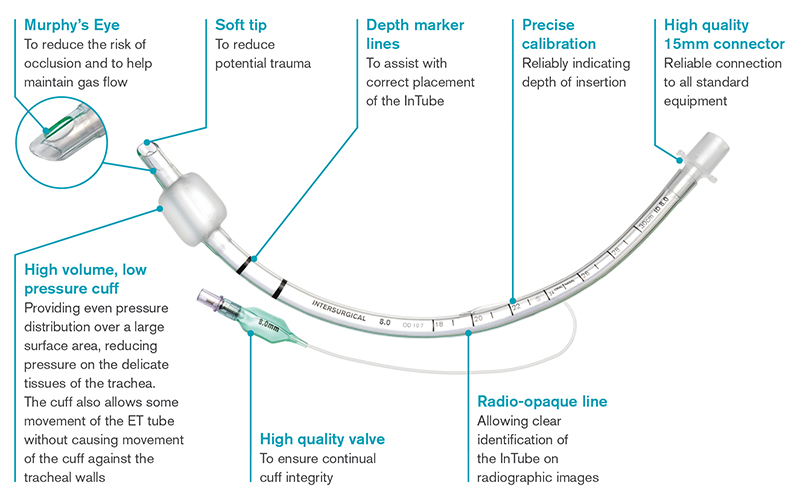
Endotracheal Tube
This method is the most efficient definitive airway management tool. It is used when; failure (or pending failure) of ventilation or oxygenation, inability to maintain or protect the airway (as in the case of unconscious patients, patients with inhalation injury or significant airway/facial trauma), potential for clinical deterioration (including in the setting of the patient being transported) and delivery of treatment. It consists of a clear tubing with different sizes equipped with a distal cuff that inflates and secures the tube within the trachea as well as protecting against blood, aspiration, gastric contents, and other fluids.
Sizing
ET tubes come in different IDs from 2 to 10.5mm and are chosen depending on the patient's body size. Adult female varies between 7.0 and 7.5mm ID while male varies between 8.0 to 9.0mm ID.
Insertion
In a prehospital setting, the use of laryngoscopes is necessary for the insertion of an ET tube. Offered in two different forms, Miller and Macintosh, they both have their own benefits. A Miller blade is a straight blade while the Macintosh is curved. Choosing between both is usually up to the physician's preference. They are both offered in size 0 to 4. Alongside this tool, is a stylet (flexible metal wire) inserted in the tube in order to give it shape as well as being used as a guide for the tube. Ventilating the patient is primordial in assuring proper tissue oxygenation before attempting intubation. Once proper ventilation is achieved, with sterile hands and suction ready, the physician needs to lube the tip of the tube using Xylocaine preferably. Positioning is an important factor in proper tube insertion, the lower part of the cervical spine should be flexed. This position allows for better visualization. With the laryngoscope, a proper technique is needed to order to obtain proper visualization, using a sweeping right to left method with the blade is the most known method. The tip of the blade is inserted on the right side of the mouth while advancing towards the tonsillar pillar. A sweeping method to the midline, sweeping the tongue left until the physician sees the tonsillar fossa. The blade is then advanced into the vallecula, between the base of the tongue and the epiglottis. Once the blade is in the vallecula, elevation of the mandible can prove to be quite a challenge, one important thing to remember is that the laryngoscope is not a lever. The physician should move the handle in the direction it is pointing at an approximate angle of 45 degrees. If the physician uses the handle as a lever, secondary injuries can occur such as facial fractures. Proper use of the laryngoscope will allow the physician to visualize the cords and allow for smoother insertion. The physician should maintain visual of the cords as the ET tube is passed through the oropharynx, it should be inserted with the cuff just past the vocal cords. A landmark for adults is the 22 cm mark which should be leveled with the corner of the mouth. Once done, remove stylet and laryngoscope. Inflate cuff with 5-10 cc’s or air, too much air can cause necrosis while too little with cause leaks. Adjustment can be done later. Confirm placement with stethoscope on the epigastric and left and right hypochondriac. Troubleshoot accordingly if needed.
Contraindications
Severe facial trauma where intubation is impossible as well as spinal immobilization that makes intubation difficult.
About the Author

NPA

OPA

Crico

ET Tube