The Cardiomyopathies
Introduction
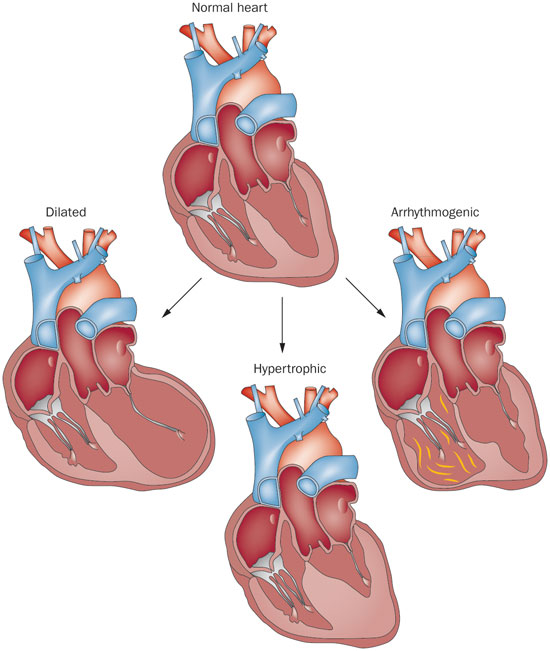
The cardiomyopathies refer to a form of heart disease that directly affect the structure and function of the myocardium. There are three widely regarded types of cardiomyopathies: Hypertrophic cardiomyopathy, restrictive cardiomyopathy and dilated cardiomyopathy. The pathophysiology of each will be explained in detail below.
Epidemiology
It is estimated that cardiomyopathy affects some 7.9 million people yearly. Hypertrophic cardiomyopathy affects 1 in 500 people while dilated cardiomyopathy affects 1 in 2,500 people.
Pathophysiology
HCM: The pathophysiology involves hypertrophy of the left or right ventricle that is usually asymmetric. Involvement of the intraventricular septum occurs often. As a result, the compliance of the left ventricle falls. This leads to an impairment in diastolic filling and relaxation. Almost 50% of these cases are genetic.
DCM: Left ventricular remodeling leads to wall thinning and a change in geometry to a more spherical shape. This leads to depressed systolic function and a fall in ejection fraction. Causes include: alcohol abuse, chagas disease, viral myocarditis and thyroid dysfunction.
RCM: The pathophysiology of this form is such that the ventricular volume and wall thickness are within normal limits, however, there is decreased biventricular diastolic volume. Causes include: amyloidosis, hemachromatosis, sarcoidosis and post radiation fibrosis.
Signs and Symptoms
The presentation of these patient generally resemble that of heart failure. Patients may complain of dyspnea on exertion, bilateral lower extremity swelling and chest pain or palpitations. A third heart sound may be heard in dilated cardiomyopathy and a fourth heart sound may be heard in hypertrophic cardiomyopathy.
Diagnosis
Workup of these cardiomyopathies include these four studies:
EKG - will generally show left ventricular hypertrophy in dilated cardiomyopathy and hypertrophic cardiomyopathy. It is usually nonspecific in restrictive cardiomyopathy.
CXR - may show an enlarged cardiac silhouette in dilated cardiomyopathy. It will be normal in hypertrophic and restrictive cardiomyopathy.
ECHO - gold standard diagnostic tool for all cardiomyopathies.
Treatment and Management
DCM
-
Those patients with newly diagnosed and/or symptomatic DCM generally require admission.
-
Furosemide and digoxin may improve symptoms.
-
Consider beta blockers, such as carvedilol, to manage tachycardia.
HCM
-
Symptomatic, unstable patients will require admission
-
The hallmark of treatment for patients with chest pain and HCM is beta blockers, such as atenolol.
-
If discharged to home, counsel patients to refrain from vigorous activity until following up with their cardiologist.
RCM
-
Consider use of diuretics to better symptom control.
- Like above cardiomyopathies, admission will be based on symptom severity, hemodynamic instability and ability to follow up with the appropriate specialty in a timely manner.