Epinephrine (Adrenalin) Notes

Pharmacologic Category
- Therapeutic: inotropics, vasopressors
- Pharmacologic: alpha and beta agonist
Indications & Dosing
- Cardiac Arrest: Asystole/pulseless arrest, pulseless VT/VF
- 1 mg (IV/IO) every 3-5 minutes until return of spontaneous circulation (ROSC)
- 2 to 2.5 mg (ET) every 3 to 5 minutes until IV/IO access established or ROSC
- dilute in 5 to 10 mL NS or sterile water
- Increases coronary perfusion pressure during cardiopulmonary resuscitation
- Bronchospasm - reversible airway disease due to Asthma or COPD
- Anaphylaxis and other systemic allergic reactions; epinephrine is the agent of choice.
- 0.2 to 0.5 mg IM every 5 to 15 minutes in the absence of clinical improvement
- Start a dirty epi drip (see below)
- Cardiogenic shock, especially if a vasodilator is added.
- Bradycardia (symptomatic; unresponsive to atropine or pacing)
- Hypotension
- 2-10 mcg per minute
- To make a dirty epi drip (great article by Zlatan Coralic, PharmD on ALIEM)
- Take code-cart epinephrine. It doesn’t matter if it is 1:1,000 or 1:10,000!
- Inject full 1 mg into a 1,000 mL normal saline bag (final concentration 1 mcg/mL).
- Run wide open until the patient’s hemodynamics stabilize.
Administration
- IV (by central line)
- Endotracheal tube (rapidly absorbed by tracheal mucosa)
- Subcutaneous
- Intramuscular
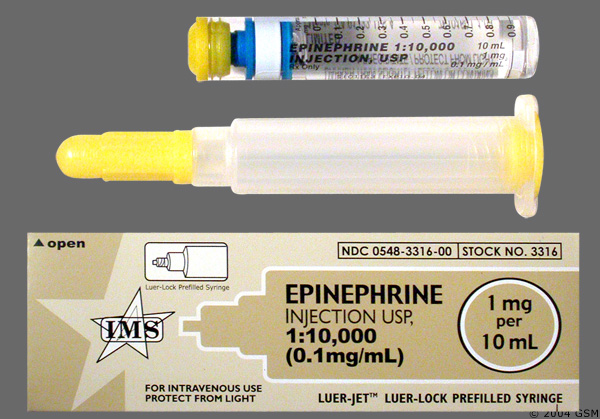
Concentration
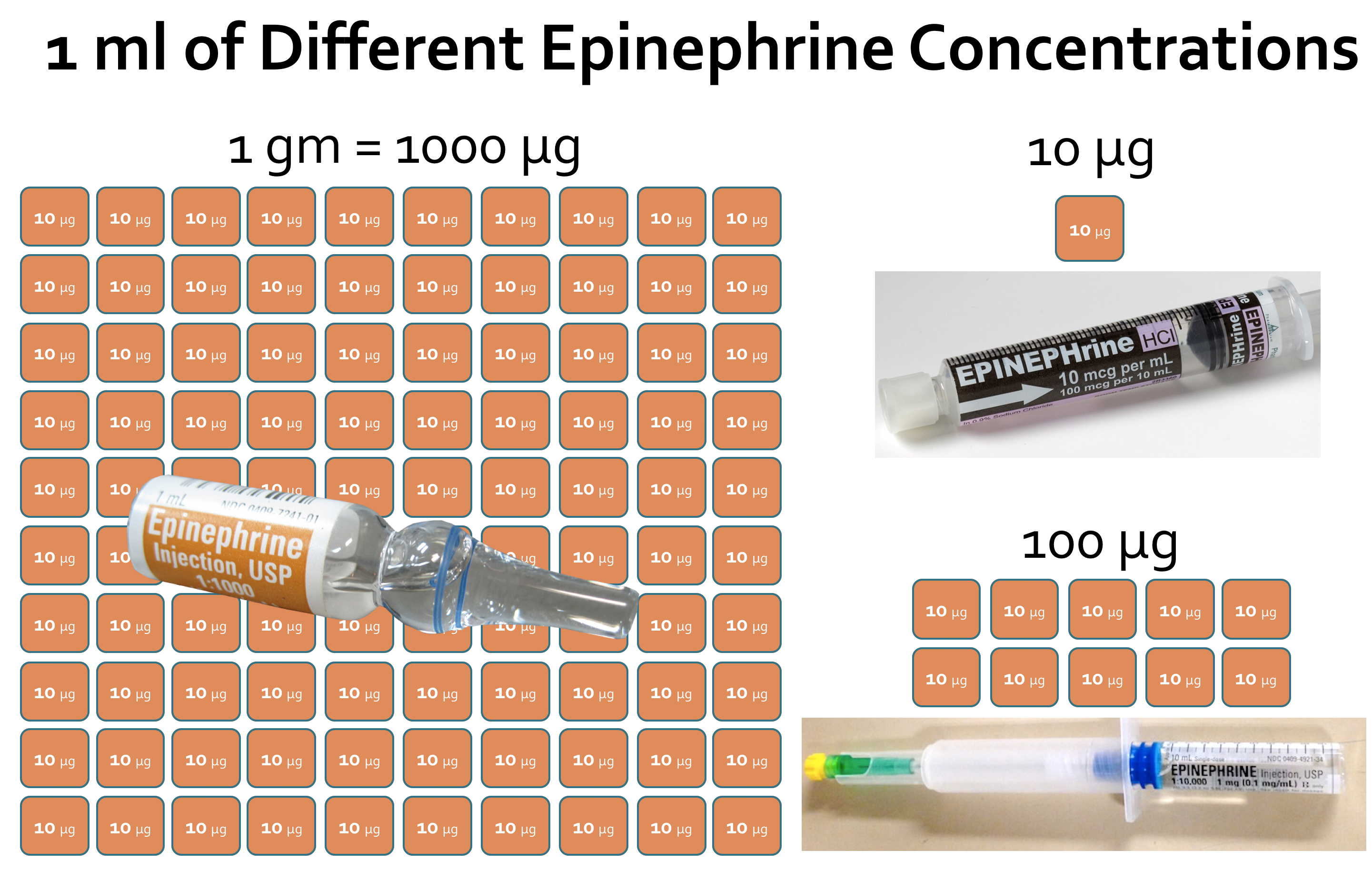
- 1:1,000 is equivalent to 1 mg/mL
- 1:10,000 is equivalent to 100 mcg/mL
Work's Consulted
- Davis's Canadian Drug Guide for Nurses
- Marino's ICU Book
Review
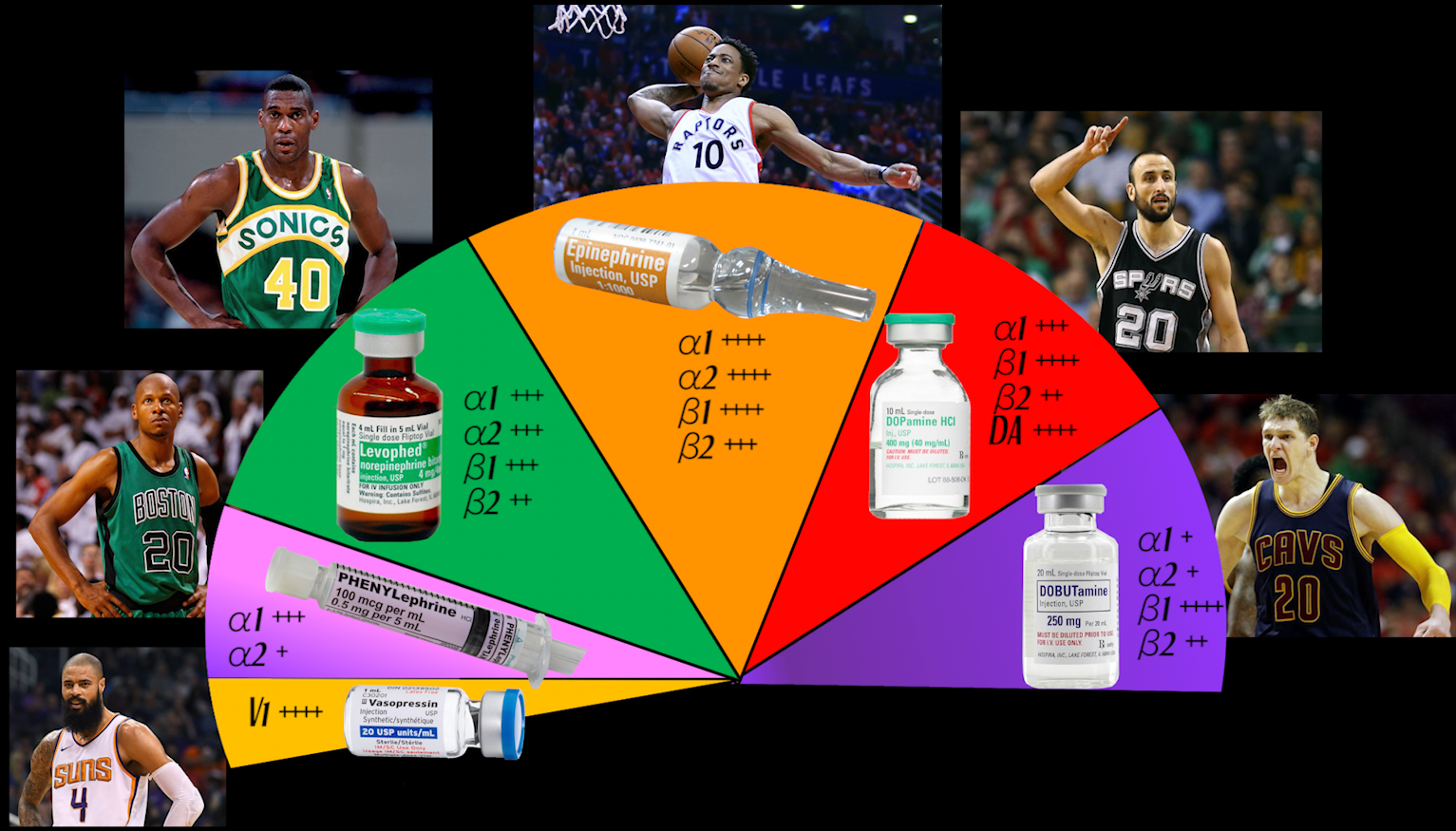
In this song, I use basketball players as a metaphor for vasopressors and inotropes used in critical care medicine. Their jersey numbers reflect their maximum dose. Their position reflects how they should be administered, central vs. peripheral. The song is filled with many homonyms, so that each time you listen you may discover something new. On the right side of the screen, I reveal these meanings as the song progresses
Discussion
What to join the discussion? Sign-up here!
The are currently no comments