Asthma Treatment and Management in the Pediatric Population

Here is what helped me get through pediatric asthma cases during my pediatric clerkship. Although my notes mostly review some of the treatment options for asthmatics in the pediatric population, I found it was important to ask these patient's or their caregivers a few pertinent questions:
- History of asthma
- Prior intubations or ICU stays because of an asthma exaceration
- Frequency of how often they've used their albuterol inhaler at home prior to coming into the office or emergency department.
- Family history of allergies or asthma.
- Their technique when using their inhaler and if they are using it correctly. Are they using their spacer if one was given to them?
The mainstay treatment was albuterol nebs +/- steroids and magnesium. The latter being reserved for patient's who have failed an initially attempt with albuterol treatment only.
Overview of Treatment Options
There are a few things you can try to treat asthmatic patient's the first being albuterol.
Albuterol Nebulizers
- albuterol x 3 q30 min (after 3, if no or minimal improvement, you can continue every 30 min or try continuous albuterol)
- can try continuous albuterol (0.5 mg/kg/hr)
- total beta agonist should not exceed 20 mg/hr
- Dosing:
- 5yo 2.5
- >5yo, 5
- Reassess at 1 hr
- neb continuous or <q2 hr --> PICU
- neb q2h --> regular hospital admission (floor)
- neb q4h --> home
- ipratropium, usually given in severe exacerbations with albuterol (250 micrograms per dose for children who weigh <20 kg; 500 micrograms per dose for children who weigh >20 kg
*albuterol 2.5/ipratropium 250 for those <5 yr old
Steroids
PO:
- Dexamethasone 0.6mg/kg x 1 or
- Prednisone 2 mg/kg LOAD --> 1 mg/kg BID for 3-5 days
IV
- methylprednisolone 2 mg/kg LOAD, MAX 125 mg --> 0.5 mg/kg q6hr, MAX 125mg
Magnesium
Given after failed initial treatment or with acute severe deterioration. I found that at this point, the patient is almost always admitted because of how severe the asthma exacerbation is. They will likely need further observation. The dose is 40 mg/kg (maximum 2 grams), in a pediatric patient.
Adjuncts
- Epi (1:1000) 0.3 to 0.5 IM
- Terbutaline 5-10 mcg/kg (LOAD), 0.4 mcg/kg/min (gtt)
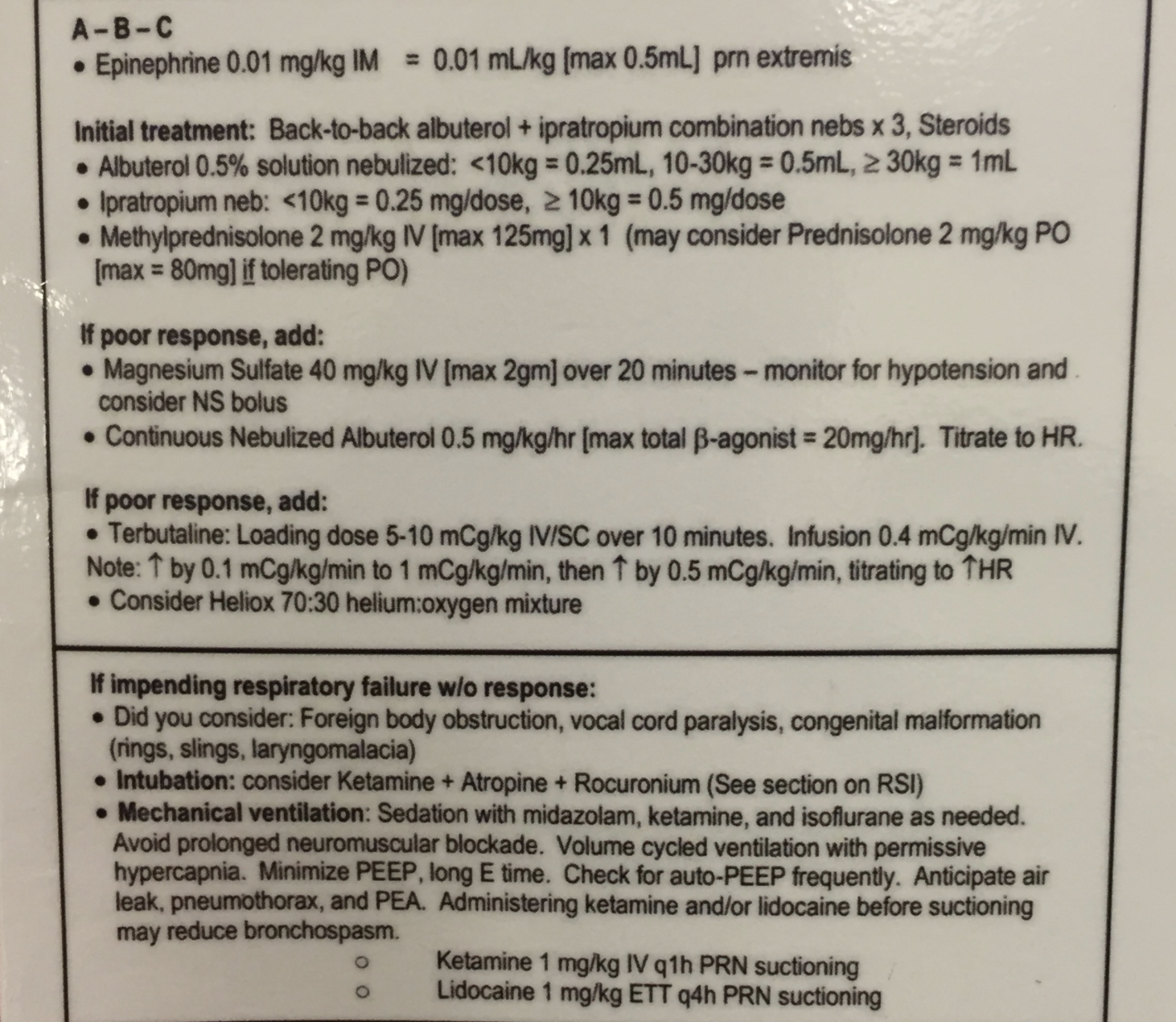
Overview
Here's a snapshot of a cheat sheet I use to keep in my pocket during rounds!